Retake
C5) Pneumonia Refractory to Antibiotic Treatment
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with fever and cough.
- Review the DDx considerations in fever and cough.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with fever and cough.
History
A 60-year-old male with progressive myasthenia gravis presented three days ago with new onset fever and cough and was started on an antibiotic for a left lower lobe aspiration pneumonia. He remains febrile with fever and cough three days later.
Physical Exam
BP: 127/70, HR 104, RR 22, Temp 40.0C, O2 saturation 88%. General: Increased work of breathing. Lungs: reduced breath sounds, decreased tactile fremitus, and dullness to percussion in left lower lung field. Remainder of exam unremarkable.
Labs
WBC: 21 x 10^9/L with left shift.
Provisional Diagnosis
Select the Dx you believe is most appropriate
Lung abscess and empyema both represent progression of a pneumonia and can explain the patient’s continued, treatment resistant fever, and leukocytosis.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
Further workup should be performed urgently in this patient with pneumonia that is not responding to antibiotic therapy.
First Imaging Study
What is the first imaging study you will order?
A chest X-ray is a quickly obtainable test that can suggest the presence of a parapneumonic effusion, empyema, or lung abscess.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
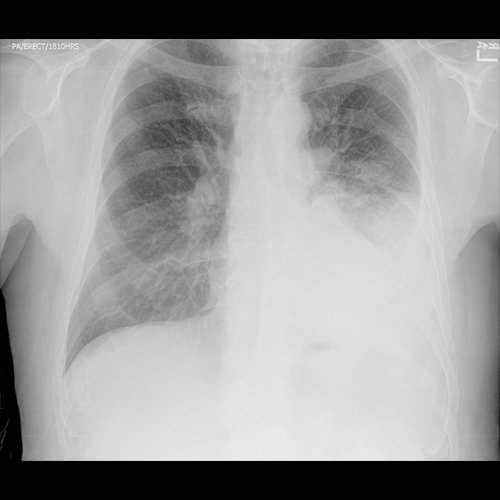
Chest X-ray
What best describes the findings on the Chest X-ray?
This chest X-ray is most consistent with a pleural effusion as the left costophrenic angle is obscured. There likely are also airspace opacities in the left lower lung indicating the underlying pneumonia.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
Sometimes, X-ray can strongly suggest the presence of a complicated pleural effusion or empyema, where it forms an obtuse angle with the chest wall and has a lenticular, biconvex shape. These findings are not evident on the radiographs. Considering the strong clinical suspicion, we should obtain a CT for further evaluation. Chest CT with contrast is preferred for evaluation of pleural effusion or empyema.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
Chest CT
What best describes the findings on the Chest CT?
The lobar pneumonia with air bronchograms in the left lower lobe is apparent. The visceral and parietal pleura are thickened due to fibrin deposition and enhance due to vessel growth. This represents the “split pleura sign”.
View the full study if you'd like to like a look yourself
Third Imaging Study
What is the next imaging study you will order?
The CT findings strongly suggest a complicated pleural effusion or empyema.
What is your Diagnosis now that you have seen the imaging results?
The thickened and enhancing pleura on imaging suggest that this is a complicated paranepneumonic effusion or empyema.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient will likely require image guided drainage for the new complicated pleural effusion or empyema.
Assessment and Plan
Please provide your assessment and plan for this patient
The patient has a lobar pneumonia refractory to antibiotic treatment secondary to newly developed complicated parapneumonic effusion or empyema. A radiology consultation is recommended for possible diagnostic and therapeutic image-guided drainage.
Lessons Learned: In a complicated parapneumonic effusion, there is bacterial invasion in the pleural space. Therefore, the pleural fluid would have a positive gram stain, low pH (<7.2), and low glucose (<60). A parapneumonic effusion is considered an empyema when there is frank pus in the drained fluid. CT with contrast revealing thickened and enhancing pleura strongly suggest the presence of a complicated pleural effusion or empyema. Loculations can be present in both complicated parapneumonic effusions and empyema.
Socioeconomic Factors: Uncomplicated parapneumonic effusions can be treated conservatively with antibiotics and serial chest X-rays if small and not leading to respiratory compromise.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Bayar Batmunh, MS - Coordinator
Next


{kind=link}
{kind=link}